

Abstract
Background:
Richter transformation (RT), also known as Richter syndrome, is a rare complication of chronic lymphocytic leukemia (CLL)/small lymphocytic lymphoma (SLL) that has an aggressive clinical course and unfavorable prognosis. The majority of these transformations occur in the form of diffuse large B-cell lymphoma (DLBCL), and less frequently in the form of prolymphocytic leukemia (PLL), or classical Hodgkin lymphoma (cHL). We examined a series of RT cases with available CLL/SLL data diagnosed at our institution between 2000 and 2018 to identify clinical/biologic characteristics associated with adverse outcome.
Design:
After searching our pathology archives between the years 2000-2018, we identified a total of 83 RT cases: 75 DLBCL-RT (including 7 PLL-RT) and 8 cHL-RT. For the purposes of this study, we focused only on DLBCL-RT cases. All clinical, demographic, and pathologic data including cytogenetics (karyotype and FISH), immunohistochemistry (IHC), and flow cytometry were collected. Data points included age, gender, CLL/SLL histology (typical vs. atypical), CD5, CD38, ZAP-70 status, CLL karyotype, FISH [chromosomes 11q (ATM), trisomy 12, 13q, 14 (IGH), 17p(P53)]. In addition, time to transformation (months), site of transformation, transformation biopsy characteristics (germinal center vs. non-germinal center, CD5 status, along with MYC and BCL2 IHC status), and karyotype at transformation were collected. For the current analysis , karyotype and FISH data were dichotomized into (complex vs. non-complex) or (abnormality present vs. absent) respectively. Limited CLL treatment data was also collected but details on performance status, stage and IPI at transformation were not available.
The clinical end point was overall survival (OS) determined as age at the time of transformation to death due to any cause, censoring patients without an event at last follow-up. Hazard ratios and 95% confidence intervals were derived from Cox proportional hazards regression models. Data analyses were performed using Stata®11.
Results:
Among DLBCL-RT patients, the median age at transformation was 66 years (range: 43-95). 87% of cases had antecedent CLL with a typical phenotype (CD5+, CD23+, FMC7-), 66% of CLL cases expressed CD38 (flow > 20% positivity) and 77% were positive for ZAP-70 (IHC). There was no correlation between CD38 expression and ZAP-70 (p=0.7). Fifty-three percent of the CLL cases harbored a complex karyotype. The most frequent abnormalities detected by FISH were TP53 aberrations (39%), followed by del13q (37%), Trisomy 12 (33%), IGH breaks (21%) and 11q/ATM deletion (17%).
Transformation occurred at median of 59 months (0-352 range) after CLL diagnosis. DLBCL-RT was non-germinal center B-cell phenotype in 85% (n=27) of cases, with variable expression of CD5 (61%), p53 (50%), MYC (83%) and BCL2 (90%). EBER was infrequent at transformation (4%; n=23). Among DLBCL-RT, a total of 29 patients died at a median of 6 months (0-58 months) after RT diagnosis.
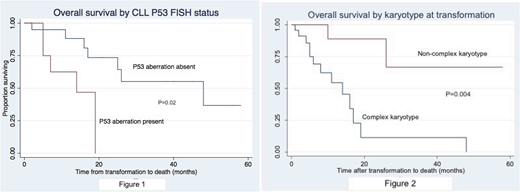
In univariate analysis, age at transformation, type of CLL (typical vs. atypical), site (nodal vs. extranodal), CLL CD38 or ZAP-70 expression did not impact survival outcome. Only TP53 aberrations by FISH in antecendent CLL (p=0.02) (Figure 1) and the presence of complex karyotype at transformation were associated with adverse survival outcome (p=0.004) (Figure 2). MYC and/or BCL2 genetic alterations at transformation did not impact outcome. In a multivariable Cox model including both CLL TP53 aberrations and complex karyotype at transformation, only complex karyotype at transformation is weakly associated with outcome (p=0.09; hazard ratio 0.14 [0.015-1.36]; 95% CI) although this analysis is limited by the number of available patients with complete data (n=17).
Conclusion:
DLBCL-RT from an underlying CLL has a poor survival outcome and only TP53 alterations in the CLL and complex karyotype at transformation impacted survival.
Stock:Jazz Pharmaceuticals: Consultancy. Riedell:Bayer: Consultancy, Speakers Bureau; Novartis: Consultancy; Kite Pharmaceuticals: Consultancy, Speakers Bureau. Smith:BMS: Consultancy; Portola: Honoraria.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal